
No Stairway to Heaven – An Unfortunate Fall Prompts Changes
On December 16, 2024, a serious accident occurred at East Midlands Airport involving a Boeing 737-8K5 aircraft, registered as G-TAWB. The Senior Cabin Crew Member (SCCM) was closing the front passenger door when the steps were unexpectedly pushed away from the aircraft. She fell into the gap between the steps and the aircraft, landing on the ramp below. She suffered multiple broken bones and had to undergo a long recovery period.
The accident happened during the turnaround of the aircraft, which was running late for its scheduled flight to Lanzarote. The SCCM had just released the gust lock on the door and was beginning to close it when the steps were moved. The dispatcher, who was still at the top of the steps, managed to hold onto the side rail to avoid falling, but the SCCM was not so fortunate. She fell to the ground, while her fellow crew members, inside the aircraft, were not even aware of the unfolding events.
“The step removal process was conducted in a way that was not consistent with the written policy and had insufficient safeguards to prevent movement of the steps with people on them or the door still open”
The investigation revealed that the steps were moved prematurely due to a procedural workaround that had been in place for years. Dispatchers, who were not qualified to operate the steps, were routinely involved in the door closure process. This practice was so widespread that it had become normalized, even though it violated official procedures. “The workaround had been going on for many years and was not limited to the staff at East Midlands. It occurred on many occasions and as such, it was hardly recognised as a workaround,” the report stated.
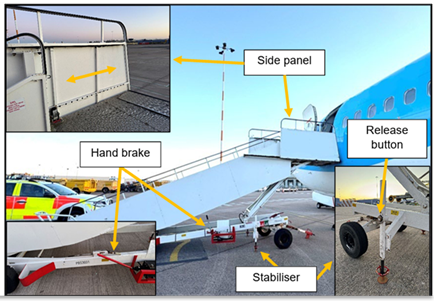
The ground handling company’s Standard Operating Procedures (SOP) required ramp staff to ensure the steps were clear, and the door closed, before moving the steps. However, the procedures did not specify who was responsible for this check or how it should be performed. On the day of the accident, multiple dispatchers were present, creating confusion among the ramp staff about whether the door closure was complete. The presence of a dispatcher at the bottom of the steps, releasing the stabilizers, led the ramp staff to wrongly assume the steps were ready to be moved. The investigation also found that the steps used in this incident were basic and lacked interlocking safety barriers. Steps with interlocking barriers prevent movement until the aircraft door is closed, and the safety rail is secured. The ground handling company was, in fact, already in the process of replacing these basic steps with the safer models, but the transition was not yet complete. “The use of the basic steps rather than those with interlocking barriers meant that the steps could be moved without the cabin door being shut,” the report noted.
The SCCM’s position at the time of the fall could not be determined, but anecdotal evidence suggested that crew members sometimes need to step outside the doorway to release the gust lock on this aircraft type. Following the accident, “the operator has amended the next revision of its SEP manual to stipulate that both feet will be kept inside the aeroplane during the door closing procedure,” the report confirmed.
The response to the accident raised additional concerns. The co-pilot called Air Traffic Control (ATC) to request medical assistance, but ATC did not fully grasp the seriousness of the situation. As a result, the airport’s Rescue and Firefighting Service (RFFS) was not mobilized as quickly as it could have been. While this delay likely did not affect the ambulance’s arrival time, it highlighted the need for clearer communication during emergencies. The report emphasized that pilots should consider declaring a formal emergency in such situations, stating, “Crews should consider that if they believe the issue would involve a 999 [112 in Malta] call if they were at home, then they should think about declaring a formal emergency.”
The accident also exposed deeper cultural and organizational issues within the ground handling company. While the company had a Just Culture policy designed to encourage open reporting of safety concerns, some staff were still hesitant to report issues due to fear of blame or punishment. The investigation process for safety events and delays was perceived as intrusive, leading some employees to prioritize on-time performance over safety. “Staff were motivated to avoid this which could be a factor influencing them to attempt to achieve on-time performance, possibly at the expense of safety,” the report observed.
Leadership and staff engagement were also identified as areas for improvement. Ramp staff at East Midlands felt undervalued and disconnected from their managers, who were based landside rather than airside. The poor state of the ramp team’s crew facilities further contributed to low morale. In contrast, the dispatch team had a highly effective airside manager and reported better cohesion and morale. The report noted, “The front-line leaders who were constantly present airside had the most influence on their staff.”
In response to the accident, the ground handling company implemented a series of safety actions. Dispatchers are now prohibited from operating any part of the steps, and only qualified ramp staff are allowed to do so. Trainee dispatchers wear different coloured high-visibility clothing to distinguish them from qualified dispatchers. Improved briefing procedures ensure that all staff know who the allocated dispatcher is for each flight. The company also increased audits and observations to ensure compliance with the new procedures. The report notes with satisfaction, “Evidence provided by the ground handling company shows that this comprehensive approach including both engagement and enforcement elements as well as continuous supervision has now achieved compliance across the UK network of over 99%.”
The operator also took action, issuing a safety notice and updating its procedures to improve crew safety during door operations. Additionally, both the operator and the ground handling company are collaborating with industry groups to share lessons learned, and develop improved procedures.
This accident serves as a stark reminder of the importance of adhering to safety procedures and addressing cultural and organizational issues that can undermine them. The changes implemented by the ground handling company and operator are steps in the right direction, but the lessons learned must be shared widely to prevent similar incidents in the future, and elsewhere. As the report concluded, “The step removal process was conducted in a way that was not consistent with the written policy and had insufficient safeguards to prevent movement of the steps with people on them or the door still open.”
The aviation industry is built on a foundation of safety, and every accident provides an opportunity to strengthen that foundation. By learning from this sad event, the industry can continue to improve and ensure the safety of all those who work in, and around aircraft.
Read the full AAIB report here: